By Dr. Michelle Arnold
Bovine Respiratory Disease (BRD) results from the mixture of host (calf) susceptibility, pathogens (viral and bacterial) and the environment to cause disease. Mannheimia haemolytica, Pasteurella multocida, Histophilus somni and Mycoplasma bovis, the most common bacteria in bovine bronchopneumonia, are opportunists that get in the lungs when the calf’s built-in defenses are down due to respiratory viruses and stress. Abrupt weaning, commingling, transportation, castration and dehorning, bad weather, overcrowding, and poor quality air and water are known to compromise a calf’s immune system. A persistently-infected (BVD-PI) calf in a pen results in continuous exposure of the pen mates to the BVD virus and a constant reduction in their white blood cells needed to fight sickness. Lightweight calves, especially those weaned on the truck on the way to the sale, that are not eating and drinking, are also at exceptionally high risk for disease and death. Metaphylaxis is one proven method to decrease sickness, death, development of chronic calves, and will hopefully improve performance.
What is “metaphylaxis”? Although this term can have a variety of different meanings, the most common one is the treatment or mass medication of an entire group of purchased feeder calves with an antibiotic upon arrival to the farm or feedlot. Some definitions also include that metaphylaxis is meant to eliminate or minimize an expected outbreak of disease, usually BRD.
How does a producer, along with his or her veterinarian, decide whether to use metaphylaxis on a group of calves? The use of too many antibiotics in food producing animals is a big concern due to antibiotic resistance development in human medicine. The decision should be made carefully. Base the decision on the risk of disease developing in that group as well as management factors such as the availability of skilled labor to identify, pull, and treat calves early during disease, and facilities to treat them in. If the risk is very high (10-20% or more will be pulled and treated) mass treatment is generally recommended to get an antibiotic on board before the bacteria have irreparably damaged the lung.
If metaphylaxis is chosen, should it be given as soon as calves arrive at the farm? The general rule of thumb is to either treat the calves on arrival or when 10% have been pulled and treated, signaling that an outbreak is likely. Timing is crucial when dealing with respiratory disease in calves. Viruses (IBR, BVD, PI3 and BRSV), stress, dehydration and other factors will damage the lung defense mechanisms and allow bacteria in the tonsils and lymph nodes to go down the trachea and into the lungs. The average time for viruses to do their damage is at day 3 after exposure then bacteria come in typically 3-5 days behind the viruses. The critical point to Figure 2. Strip grazing stockpiled grass is accomplished by starting at the water source and allocating only enough pasture understand is the battle for the lungs must be won in the first 10-14 days after exposure or admit defeat. This brings up the next set of questions: when were the calves first “exposed” to respiratory viruses and do they have any vaccination protection? As an example, unweaned calves that were rounded up and taken to the sale barn the night before the sale may have 24+ hours of bawling, walking in a dusty pen, coughing and breathing on each other and the cattle in the adjacent pens, drinking from watering troughs that are shared with other cattle or perhaps they won’t drink at all. Many (most) of these calves will not have received a respiratory vaccine prior to sale and their dams probably did not either. At the sale, these calves are then mixed and matched with others to make load lots so now the stress of commingling is added to the mix of risk factors. By the time the calves reach their final destination, they may have accumulated 24-48 hours of exposure or sometimes much more. The bottom line is to always consider how long it has been since that calf left his or her normal routine; the longer this time, the sooner you need to mass treat. In addition, if castration and multiple vaccines are given at arrival, this adds another layer of difficulty in the fight against respiratory disease. On the other hand, calves purchased that were weaned and preconditioned probably do not need metaphylaxis on arrival but could need it later if a respiratory break begins.
Which antibiotic is best for metaphylaxis? First and foremost, there are only a handful of antibiotics approved for metaphylaxis. Excede®, Nuflor®, Draxxin®, Zactran®, Zuprevo®, Micotil®, Advocin® and Baytril® are allowed for BRD “control”. The decision on which one to use and how long to wait before pulling cases should be made with the veterinarian who prescribed it. The conventional wisdom used to be to treat all calves first with the cheapest broad-spectrum antibiotic (such as LA 300) then move to stronger and more expensive drugs each time the calf is pulled. The problem with this method is that by the time a producer reaches for one of the high-powered drugs, it is too late and the damage to the lung is already done. Getting an antibiotic labeled for control of BRD gets a proven, effective drug into the lung tissue while there is still time before the severe inflammation keeps the drug from getting to its destination.
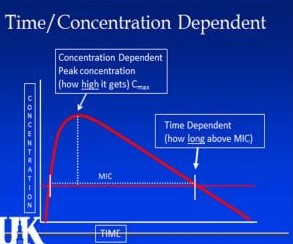
Figure 1: The “MIC” is the “minimum inhibitory concentration” or the minimum level of the drug needed to fight bacteria.
Why do some calves respond to metaphylaxis while others have to be pulled and treated again? It is easy to see why successful treatment of bronchopneumonia is not simply a matter of grabbing a bottle of the latest and greatest antibiotic, shooting it in the sick calf and waiting for the magic bullet to take effect. Instead, full recovery is a joint effort between the calf’s immune system and the selected drug to stop the growth of bacteria and destruction of lung tissue. Antibiotics are designed to hold the bacteria “in check” and give the calf’s immune system time to gear up and effectively fight the disease. Treatment failure may be due to calf factors including overwhelming stress, concurrent infection with BVD, or nutrition-related factors such as trace mineral deficiencies or subacute ruminal acidosis. Sound nutrition and management, especially around weaning, will substantially increase the response to antibiotics. Calves vaccinated 2-3 weeks pre-weaning against respiratory viruses are known to respond faster and better to antibiotic therapy if needed. A good environment with plenty of space, clean water and bunk space reduces stress. Quick identification and removal of PI calves is through a simple, inexpensive ear notch skin test. Trace mineral deficiencies can be addressed immediately with an injectable trace mineral while calves are transitioning to a trace mineral mix. Keeping high quality, leafy, green, palatable grass hay available is the best way to start them eating. Treatment failure due to human errors may include poor timing, use of the wrong drug, improper dose or route of administration, or mishandling the drug itself. The most common error, by far, is failure to recognize a sick calf. Timing is crucial; if calves are treated early during disease, almost any antibiotic will work. Conversely, if calves are treated late during the disease, nothing will work. In addition to timing, dosage is crucial because antibiotics work by different mechanisms. Figure 1 graphically displays the difference between antibiotics that are considered “time dependent” (effectiveness depends on exposure to the drug for a certain length of time) versus “concentration dependent” (bacteria must be exposed to a high concentration of the drug). If label directions are not followed and only a partial dose is administered or perhaps a second dose is required but not given, the drug is unlikely to work effectively because it cannot reach the necessary minimum target concentration. Selection of the best antibiotic class or “family” is an equally important success factor. Figure 2 is an illustration of the mechanisms antibiotic classes use against bacterial cells. Beta-lactams (penicillin, Excede®, Naxcel®, Excenel®) cripple production of the bacterial cell wall that protects the cell from the external environment. Aminoglycosides and Tetracyclines (LA-300®, Biomycin®, and many others) interfere with protein synthesis by shutting down the machinery in the ribosome needed to build proteins. Macrolides (Draxxin®, Micotil®, Zactran®, Zuprevo®, Tylan®) and Chloramphenicol derivatives (Nuflor®) also interfere with protein synthesis although at a different location on the ribosome. The Fluoroquinolones (Baytril®, Advocin®) block genetic replication by interfering with DNA and RNA synthesis. Why is this information important? If a calf requires retreatment, selection of an antibiotic from a different class will attack the bacteria through a different route and often improves treatment response. Another good example is treatment for Mycoplasma bovis, a bacterium frequently found in chronic pneumonia cases. It has no cell wall so treatment with a Beta-lactam (such as penicillin or Excede®) will prove absolutely useless. A veterinarian is well-trained in antibiotic selection and is the best source of information when choosing therapy. Another issue that may affect success is mishandling the
product; an antibiotic that gets too hot or freezes will inactivate the drug in most cases. Sometimes treatment failure is not a “failure” but rather an inability to recognize recovery. A calf that is eating, drinking and looks better after treatment but still has a slight fever often just needs time to fully recover since fever is one of the last clinical signs to disappear.
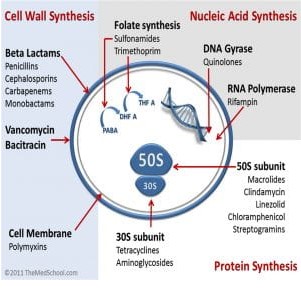
Figure 2: Drawing of a bacterium illustrating the ways different “classes” of antibiotics fight against them.
Strategic and correct use of antibiotics will continue to be of importance for the cattle industry from this point forward. Metaphylaxis is one method to head off a likely respiratory break, especially in highest risk calves. In addition, careful attention to timing of treatment, drug selection, dose, and handling of the product will reduce the human factors that contribute to treatment failure. Calf factors including overwhelming stress, infection with BVD, environmental or nutrition-related disorders must also be addressed in order for the calf’s immune system to work with the antibiotic to stop disease progression.
Source : osu.edu